
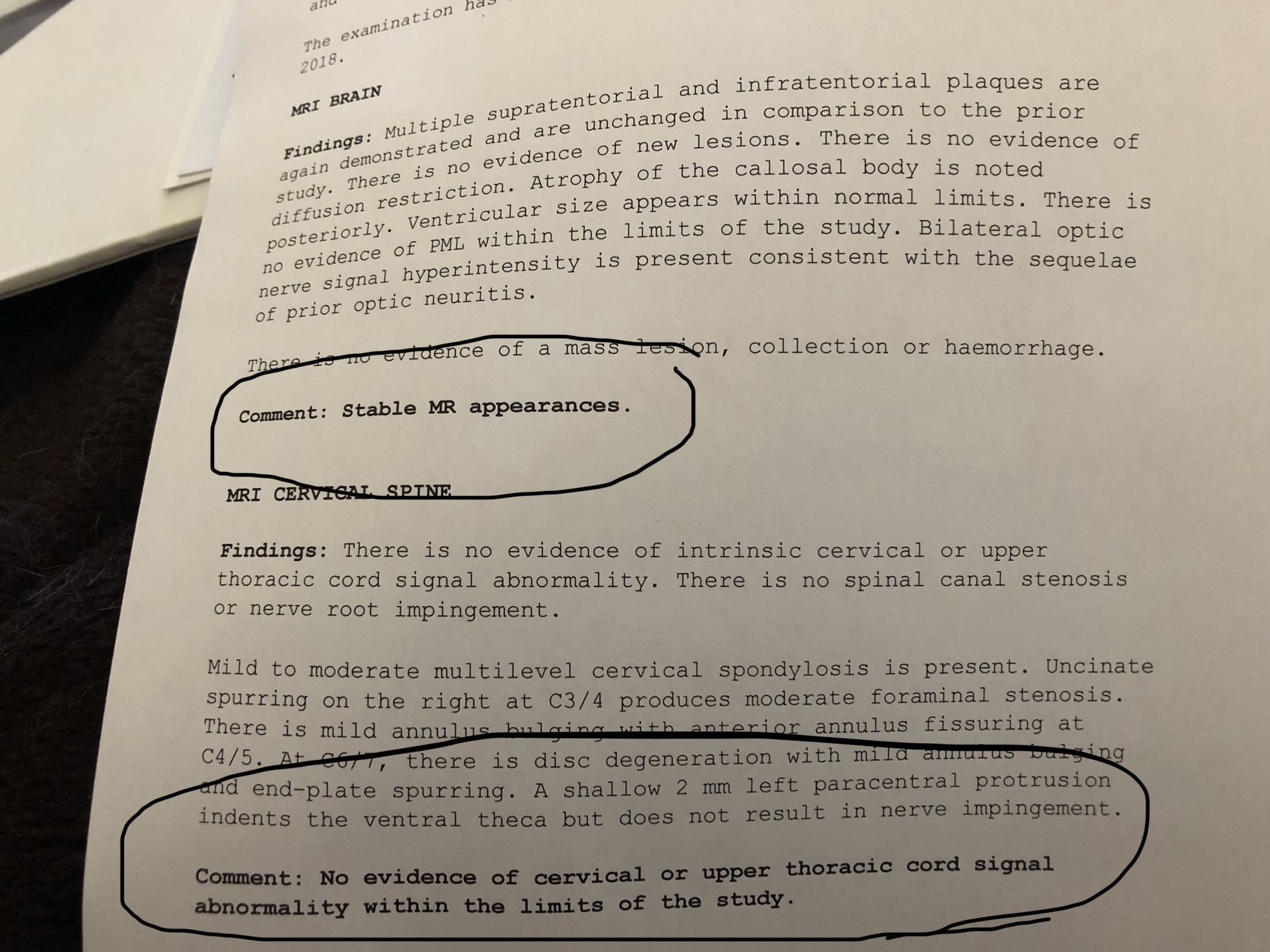
The results from my first MRI since Moscow are in. They show no change, which is exactly what I had expected. As I had no active lesions i.e. no active current attacks being made by my immune system on the myelin sheath of my nervous system, there was no sign of change. However, the Russian viewpoint is that there is inflammation and attack ongoing at cellular level, which does not show up on an MRI, however is halted when the treatment is carried out.
However, as I’ve stated before, I am seeing ongoing improvements. Therefore I am getting much more cautious about being MRIs as the only tool to use for MS. I’m going to quote some paraphrased words by one of the guys on the FaceBook forums, while I am unsure if I completely agree he has some very good points.
“MRI lesions – This post is about the important topic of MS lesion activity of MS patients seen under MRI imaging and associated HSCT effectiveness of which there is substantial confusion … I’ll spell it out here. . . .
First of all, inflammation (as evidenced by lesion activity in MRI imaging) is NOT required to experience benefit from HSCT. It’s true that a greater percentage of the HSCT treated population that has such inflammatory activity indication will fare better with successful post-HSCT outcome results, but by no means does this mean that patients with no identifiable inflammation (mostly progressive MS patients) will not benefit from HSCT. It is important to remember that lesion activity as seen under MRI is a “consequence” of MS, not a “cause.” Lesions are a symptom of MS, just like any other clinical symptom. Claiming that only MS patients with lesion activity will benefit from HSCT is just like saying that only MS patients that have optic neuritis (or any other specific MS symptom) will benefit from HSCT. That’s complete hogwash!
People (including most doctors) place waaaaaaaaaay too much overemphasis on MRI lesions. Because lesions are a consequence of MS and are themselves not a cause, lesions should be considered a “symptom” of MS just like any externally evident symptom of MS. Lesion activity seen under MRI correlates poorly with actual clinical disability, at best. Some people are “sub clinical” and have massive lesion loading seen under MRI, yet have absolutely no outward clinical signs or symptoms of MS. And some people are “hyper clinical’ and have absolutely no lesions seen under MRI yet have very severe clinical disability. MRI imaging is a notoriously unreliable measurement of MS disease activity. Outward clinical symptoms are the only manifestations that should be driving treatment decisions about MS. (I wouldn’t care if I had a million lesions in an MRI brain scan. But I would care if I could walk, or not of which there is little correlation with an MRI image.) So what is the purpose of having so many MRI scans as an MS patient? Such imaging modality offers little or nothing in the way of useful treatment decisions and offers absolutely no change in disability status over the long run in the end. Doctors should be treating “disability,” not “lesions.” …
Only a dysfunctional neurologist with poor skills as a neurological medical professional would be happy that a patient has no lesions, but still continues to clinically worsen in disability status. Because lesions seen in MRI images are so weakly correlated with actual underlying MS disease activity, using lesions as the focus of treatment is meaningless and ultimately futile. The fundamental bottom line is that in most patient treatment cases HSCT halts the underlying MS disease activity & progression, irrespective of presence or absence of MRI lesion evidence. Don’t just believe it when told otherwise. Ask for evidence. And the evidence supports what I have stated here.”
OK a long read, but my neurologist still refuses to agree that the mounting evidence is promising for AHSCT, even with consistent results of improvement at best and halting of progression for a high percentage. Reason – because there is no change to the MRI. Given the results are based on properly controlled trials, with blinded neurologists assessing the patients, so they don’t know if they are assessing someone who has had the treatment or someone who is on the drugs, I cannot understand his reluctance.


And for something much lighter, this weekend we went to see a really good band, the Melbourne Ska Orchestra in the city. A meal on Elizabeth Quay, a couple of sparkling wines, and great seats watching a great fun act … a great way to spend a Saturday night.

